
The Long Distance Runner
The following is a case study. Details have been left out in order to maintain patient privacy.
I wanted to share a case study that involves our new BioMechanics Lab! It has been an interesting progression so far and is still evolving as we go. I had a patient referred to me for a full running analysis. The patient had been experiencing chronic ongoing low back pain following long distance runs. They have had physical therapy care in the past that included hands-on therapy as well as strengthening and mobility-based rehab. Due to the lack of response from their rehab they had stopped running for the time being.
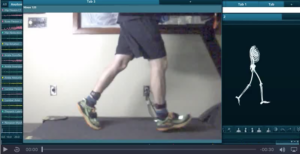
The first step was to hooked up the patient to a 3D mapping joint-capture system and performed three separate running tests. Each test has different speeds relative to the patients’ regular running program. In combination with the pressure-plate treadmill, the 3D mapping gave me insight as to how they looked while running. This data picked up on issues that would be hard to find without this equipment.
What I discovered was a significant lack of pelvic control in the form of a bilateral pelvic drop. I also saw increased rotation in the low back, decreased movement in the upper back, as well as increased vertical ground reaction forces especially upon initial contact. Taking into account their history and current presentation, addressing these issues is the first place to start their rehabilitation.
My initial plan for this patient was, to begin with, a course of gait retraining along with biofeedback training utilizing our surface EMG technology.
At the inital visit we used LED sensors placed on the wall in front of the patient to cue for their increased hip adduction during the swing phase. This immediately was helpful in addressing their pelvic drop but was very taxing on the patient’s endurance.
How did we follow up with this data?
During the follow-up appointment, we added two sensors to the back side of their pelvis and cued them to run while keeping the sensors even. This was very difficult and frustrating for them to perform. We saw a significant decrease in the ground force being absorbed (which was a good thing for them!). At the next two visits, we stuck with our initial cue of trying to correct the increased hip adduction. While this was tiring for the patient, they began to become comfortable with the change. When in the initial stage, we included sEMG biofeedback training. This was to teach the patient proper motor control of their hips/gluteals. Again, this was difficult but beneficial for them during the beginning learning process.
At the time of this write-up, the patient is halfway through their recommended treatment plan and has yet to have an episode of low back pain. While everything is under very controlled scenarios, running at controlled speeds and having the assistance of biofeedback in a lab setting, the results are promising so far! They were having episodes of pain after every run previously, so being able to run, even for 20-30 minutes, has been very exciting.
Dr. Alex Svac